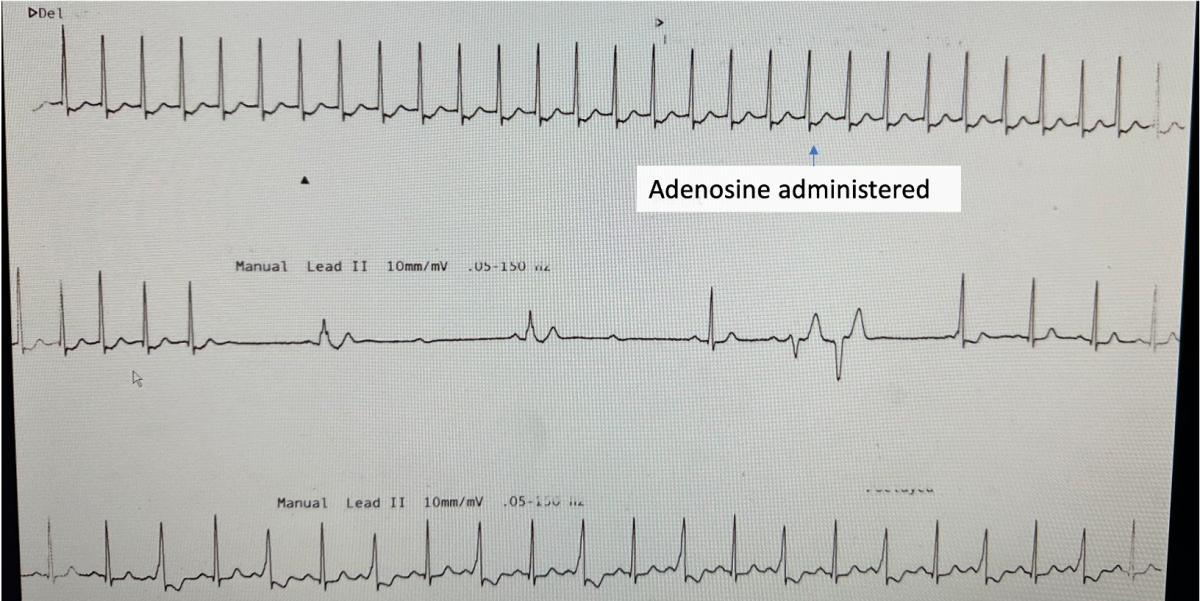
A 19 year-old woman presents with palpitations. Continuous rhythm strip post adenosine is shown. What is the likely mechanism of tachycardia? Does this patient need an urgent ablation?
provided by A/Prof Alex Voskoboinik
The Answer
A short RP supraventricular tachycardia is shown initially. Adenosine blocks the AV node and results in termination of tachycardia. This is suggestive of either typical AVNRT and orthodromic AVRT. One notes that the tachycardia terminates with an ‘A’ (seen immediately after the last QRS of tachycardia which would further rule out an atrial tachycardia – where the last abnormal beat is usually a QRS complex; moreover atrial tachycardias are only rarely adenosine sensitive).
Immediately after the tachycardia terminates, the AV node is fully ‘blocked’ and the sinus beats are only intermittently conducted to the ventricle, but down an accessory pathway. These wide complex beats are ‘fully pre-excited’, but some p waves are blocked suggestive the pathway has weak antegrade conduction properties. In the bottom row where adenosine has worn off, one can see that only every second beat is pre-excited (these beats are a fusion of nodal and antegrade pathway conduction) again confirming that the pathway has weak antegrade conduction with a ‘long refractory period’. Hence this would be considered a ‘low risk’ pathway as it is unlikely to be able to conduct AF at rapid rates (which is what can lead to degeneration to VF in patients with WPW). While catheter ablation for SVT should be considered on symptomatic grounds, there is no indication for urgent ablation of this low risk accessory pathway on prognostic grounds.